|
As my independent study comes to a close, I've reflected a bit on what I've gained from the experience, and I'm increasingly realizing that I learned a tremendous amount. Inevitably, my experience differed considerably from my original expectations that I lead out in my independent study form several months ago, because I ended up only briefly visiting some of my goals, tremendously expanding upon some of my goals, and accomplishing things I hadn't even expected. To guide my reflection, I'll first reference each goal I wrote down and analyze my experience with it.
My first goal in the independent study form was to perform hands-on neurosurgery techniques with Spine STUD models. I did indeed get to do this, multiple times! Dr. Bohl was kind enough to take some time to show me how to insert pedicle screws, which are screws onto which a titanium rod is secured to straighten out a person's spine. Dr. Bohl also showed me how to do a laminectomy, which is a fundamental surgery in which a vertebra is removed to reduce pressure on the spinal cord. Unfortunately, I didn't have time to record myself doing these techniques, because Dr. Bohl came to the lab to show me these techniques between his own real cases, so we didn't have much extra time. Although I don't think I could confidently perform these surgeries on a real patient just yet, I do feel like I have a much better sense of what it feels like to perform a surgery. There is a tremendous amount of focus, coordination, and precision required, which I now have a greater appreciation for. I also got a taste of the "surgery flow" state that comes from tremendous engagement in the present moment, which is what allows second year residents to successfully perform surgery on 4 hours of sleep for weeks on end. Of course, this state of flow is also what motivates surgeons to continue pursuing surgery in the first place, and I have a much more visceral understanding of the excitement of "surgery flow" than I did before. My surgical experience wasn't limited only to what Dr. Bohl showed me, however; I also got to perform surgical techniques completely independently on the models that I was constructing. I had to learn to use an ultrasound effectively, which is an essential tool that allows a surgeon to get a preview of the regions they will operate on. In addition, I had to learn how to make a local anesthesia injection while using the ultrasound to guide my needle, which takes practice. I ended up applying these surgical techniques many times on my own models as I tested them, and I even had to modify the techniques to best suit the imperfections of my models. For each model I made, I looked closely at its construction, and I used my understanding of ultrasounds, anatomy, and the surgical techniques to make a plan that was effective for that particular model. After each trial, I evaluated the effectiveness of my procedure, and I used this information to plan future trials more effectively. My second original goal of my independent study was to collect and analyze data about my experience with the Spine STUD models. My accomplishment of this goal was slightly different than I had expected it to be, but I still accomplished all components of it. Given that Dr. Bohl spent much of his day in the operating room, he didn't have time to show me a sufficient number of surgical techniques to allow for meaningful data collection of my surgical performance on the models. (It may sound like I never really got to see Dr. Bohl because he was in the OR all day, but I actually talked with him extensively while in the car, while at home, and while walking through the halls of the hospital. It just so happened that I was usually in the lab–where the models are–at pretty much the same time he was in the OR most days.) However, I got to collect plenty of data about a different project: designing an ultrasound/injection compatible model of the lumbar spine! I didn't know I was going to get the chance to work so deeply on this project, and I enjoyed it tremendously. In the process, I designed countless experiments about how to design a working model, and I ended up collecting almost 40 pages of qualitative, quantitative, and photographic data on my results. As is inevitable in science, I made many errors, and I learned from these errors and am now able to construct experiments in the real-world more effectively than I was at the beginning of this independent study. I feel very satisfied that I collected meaningful data, which is exactly what I had originally hoped to accomplish. Another component of the above goal that I ended up accomplishing in an unexpected way was data analysis. I'm currently learning data science, and I love working with big datasets. Although I didn't end up analyzing data on my experience with the models like I originally expected, I got the chance to analyze a much bigger dataset: a medical dataset with data on every surgery performed at Barrow between summer of 2017 and 2019. I got to apply the very tools I've been studying on my own for months, including python and the pandas library for python, to a real world situation, which was extremely exciting! In addition to analysis and manipulation, I conducted the first key step of the data science process, which was having conversations about the data to understand it before analyzing it. I talked with Dr. Sheehy, the doctor for whom I was analyzing the data, about the meaning of each row and column and the best questions to ask of the data before writing a single line of code. After this real-world data experience, I feel much more familiar with executing the steps of the data science process, including discussing the data, planning the questions to ask the data, manipulating the data, analyzing the data, and presenting the results, all in a real-world situation. My third goal was to write a formal report of the data I collected and prepare it for publication. Most of the work I did in the lab will likely be patented, so I can't publish the nearly 40 pages of data I collected and the summary of it that I wrote. However, I got to write the entire methods and results sections of a small study with Dr. Bohl, which is almost ready for submission to a scientific journal. After discussing this study and writing part of it, I feel much more familiar with the process of writing a study and confident that I have the fundamental skills to help plan and write future studies. My fourth goal was to shadow Dr. Bohl in the clinic to understand the daily life of a neurosurgeon, and I accomplished this goal almost exactly how I expected. Every morning, I went with Dr. Bohl to rounds from around 6-7:30, and I got to see surgeons analyzing x-rays, CAT scans, and MRIs. During rounds, I also got to follow Dr. Bohl and his junior resident to check on patients in the intensive care units (ICUs). In addition, I went with Dr. Bohl to meetings with the attending neurosurgeons, in which they discussed the results of the residents' surgeries and how they could be improved. Another type of meeting I got to see was called journal club, in which a group of neurosurgeons got together to discuss new neurosurgery research. I also learned a lot about neurosurgery through simply talking with Dr. Bohl. He told me all about the med school/residency/attending process, the hours that each type of neurosurgeon works, what he spends most of his day doing, flexibility within neurosurgery, how call works, and many other things. Finally, I got to see firsthand how challenging call can be when Dr. Bohl was suddenly informed that he had to go back into the hospital on Saturday to conduct an emergency right before we were all about to eat dinner. I spend lots of time evaluating the lifestyle of a neurosurgeon and whether that's a lifestyle I'd want to have, and I now feel that I can make a much more informed choice about whether to go into neurosurgery. My fifth goal was to plan the development and assembly of new Spine STUD models, which I got to expand far beyond what I was expecting. As previously mentioned, I spent hours each day in the lab conducting experiments and working on new models, and I was working largely independently, making my own hypotheses and designing my own experiments. Sarah McBryan, the senior lab engineer, helped me get started by teaching me the basics of working in a real world lab, and I can use this knowledge as a starting point for working in any other lab. In addition, Sarah gave me some excellent life/career advice. I now feel much more capable in a lab, and my development and experimentation skills have improved tremendously from the beginning of my independent study. Finally, my sixth goal was to try the neurosurgery techniques on a cadaver. Unfortunately, we weren't able to get and operate on a cadaver, but the wonderful, unexpected experiences I had with goals I hadn't even foreseen more than make up for not getting a cadaver. Another thing I got to see that I learned a tremendous amount from was a business meeting between Spine STUD and patent attorneys. As discussed in my blog post for that day, I got to learn about the process and importance of patenting a new invention, and I now have a better sense of what being a patent attorney involves. Although this isn't directly related to neurosurgery, it's certainly relevant to neurosurgery, because neurosurgery involves tremendous amounts of technology, which has to be patented. This was another unexpected and very valuable piece of learning from my independent study. Overall, I've grown tremendously from this independent study, and I'm extremely grateful to Dr. Michael Bohl, Sarah McBryan, Jessica Bohl, and everyone else who helped make this valuable experience possible!
0 Comments
My main activity today was analyzing the surgery data that Dr. Sheehy sent me. My first task was to add a column to the entire dataset that contained the share of each surgery that overlapped with another surgery that the same doctor was doing. For instance, if surgery A started at 7 and ended at 8, and surgery B started at 7:30 and ended at 9:30, and both surgery A and surgery B were supervised by the same attending, then the overlap_share column value for surgery A would be 0.5, and the overlap_share for surgery B would be 0.25. My job was to use the start and end times of each surgery and the name of the doctor who performed each surgery to make a new column for these values with every row in the dataset.
I started by converting the start and end times to python datetime values, which represent moments of time in a way that the computer can easily understand. One big benefit of datetime values are that subtracting one from another results in a timedelta value, which is a value that represents a difference between times. It's easy to get the number of seconds from this timedelta value, so I made a new column called duration_secs with the duration of each surgery. The next thing I had to do was find out when the doctor's next surgery started and when the doctor's previous surgery ended. These values allow the overlap share to be discovered relatively easy. I began by generating a list of each individual doctor in the dataset. I then looped through each of the doctors in this list, selecting a subset of the dataset that only had the surgeries that one doctor did on each loop. I had to think for a while about my next step, because it's best to use a type of operation called a vectorized operation when working with the tool that I'm using in order to make computations as fast as possible. To make the next_start column, I ended up duplicating the start column, taking the top value off, and moving all the values up one row. I did a similar thing to make the previous_stop column. Once I had these two essential columns, I isolated the surgeries that overlapped with others done by the same doctor by finding out whether the difference between the start of the next surgery was before the stop of the current surgery, or vise versa. For these rows, I used the timedelta technique mentioned above to determine the time that each surgery overlapped with another. Finally, I divided the overlap column time by the total time of the surgery to get the overlap_share column! This process sounds relatively streamlined as I summarize it, but just like doing science in the lab, manipulating data takes lots of trial and error, especially for a person like myself who is in the process of learning these tools. I think this project helped me become considerably more fluent with the tools I used to do it. I didn't get the chance to do any statistical analysis or make machine learning algorithms on this data, but I still enjoyed manipulating it, which was all that needed to be done here. Good data manipulation skills are critical for any other data skills, because it's important to be able to get the data into any format you can possibly think of to make it as easy as possible for models to handle. Good data manipulation skills also allow the data to be made into a more human-readable and understandable format, as I did here. All parts of working with data are important and interesting in their own ways. Dr. Sheehy was telling me about his own attempts to analyze this data, and he said that he had successfully devised a way to analyze this data in excel, but the algorithm that he created wasn't very efficient; it took a whopping 48 hours to run! This is a good situation in which non-graphical data analysis tools, like python and pandas, are more effective than excel. This is true for a variety of reasons. One reason this is the case is that pandas supports vectorized operations, which make code much faster. Another reason this is the case is because excel had to spend time graphically loading all data that it analyzes, while python can take care of everything you tell it to do behind the scenes. This make code exponentially faster, because it's not necessary for the computer to waste processing power graphically loading things as it does them. Big datasets are an essential part of the medical field, and I enjoyed my chance to work with them! I plan to stay in touch with Dr. Sheehy to help him with any other analysis that he could use help on. I spent most of today working on a study that I'm helping Dr. Bohl write. He introduced this study to me when I was in Phoenix, and I planned to work on it after I got back. This study involves a treatment called lumbar interbody fusion (LIF), which is a procedure in which a lumbar spinal disk is removed so that two vertebrae can be fused together. This process is useful when a disk is causing pain by pressing on nerves, which is a common problem. There are several ways to do this surgery. The traditional method involves opening a patient's entire back to access the lumbar spine, which requires cutting through lower back muscles. This can sometimes lead to lower back pain, so another less invasive method also exists to perform this surgery. This minimally invasive method involves cutting through the side of a patient's abdomen with a relatively small incision, which is sufficient to reach and remove a spinal disk.
However, both methods of surgery are associated with a risk of a condition known as adjacent segment disease (ASDz). ASDz occurs when adjacent segments begin to degenerate after the LIF procedure is completed, as ASDz can be painful and dangerous to patients. There isn't consensus in the scientific community about exactly what causes ASDz. Some scientists argue that ASDz is caused by natural aging-related changes in the spine that are already present in people who tend to need LIF, while others argue that the LIF process itself causes ASDz. Incidence rate of ASDz hasn't been well studied, which makes LIF a somewhat controversial treatment. Doing studies on surgical procedures is often challenging, because datasets are usually quite small for surgeries compared to other types of medical treatments. The dataset in the study I'm working on only has 26 cases (each represented by a row), which means that this study isn't super informative on its own. Dr. Bohl explained that studies like these are basically designed specifically to be meta-analyzed. When 10 or 20 teams write similar studies with a few dozen cases each, a researcher can analyze the big dataset that results from combining these studies to get more meaningful statistics and stronger insights. I'm responsible for the methods and results sections of the study, and I have the dataset for the study. For the methods section, I described in detail every piece of data that was collected on the patients, including details about the type of surgery, the dates of the surgery and follow-ups, data on the patient's subjective assessment of the surgery, and crucially, ASDz incidence. I also highlighted that this was a retrospective chart review, as opposed to a prospective chart review. A retrospective chart review involves asking questions about medical data that already exists, while a prospective chart review involves asking questions, then collecting data after the questions are completely formulated. Retrospective chart reviews are usually more realistic to carry out and can be performed on larger, pre-existing datasets, but seeing the data before asking questions can bias the questions towards topics that the data answers in a desirable way. A prospective chart review is more difficult to carry out because the researchers must collect the data themselves after asking the questions, but it makes likely a less biased outcome. It is important to be highly conscious of potential bias in the questions you ask of the data when conducting–and interpreting–a retrospective chart review, so I found it important to highlight this detail of the study in the methods section. In the results section, I discussed most of the content of the data we collected. I did some simple statistics on the numerical values, though I had to be conscious of the fact that on such a small dataset, some statistics such as the standard deviation aren't meaningful. Since this study hasn't yet been published, I can't go into detail about the findings. Once I finished the draft, I emailed my first draft to Dr. Bohl, and I'll edit the study in the next few days to incorporate his feedback. Last night and this morning, I had the privilege to speak with three of the most prominent neurosurgeons in the world. One of these surgeons was Dr. Michael Lawton, the lead neurosurgeon at Barrow, who specializes in brain surgery (as opposed to spine surgery, which is what Dr. Bohl specializes in). I also got to speak with neurosurgery legend Dr. Robert Spetzler, who has contributed tremendously to the development of the entire field of neurosurgery. In fact, Dr. Spetzler regularly appears in summary articles like this one that list the most innovative neurosurgeons alive today. Finally, I got to meet Dr. Mitchel Berger, another highly prominent neurosurgeon who is the chair of the neurosurgery department at UC San Fransisco. Barrow and UC San Fransisco are two of the best neurosurgery residency programs in the world, so I'm honored to have had the opportunity to talk with the chairs of both programs, in addition to a legend in the field of neurosurgery.
I also got to see a fascinating talk by Dr. Berger on his innovative ways of performing neurosurgery. The focus of the talk was a striking technique that involves keeping the patient awake during neurosurgery! The purpose of this technique is to map regions of the brain during surgery to determine the best path to a brain tumor. During this procedure, Dr. Berger removes part of a patient's skull while they are still awake and conscious (but physically stabilized and under powerful local anesthesia, of course). He then stimulates various parts of the exposed brain using a very subtle electrode and asks the patient where they feel a tingle in their body. He uses their verbal answers to determine which parts of the brain are directly connected to each body part in his individual patient. During this procedure, he also tests language function by location. He shows the patient a continuous stream of simple images on a computer screen, which the patient is instructed to read out as they appear. As the patient is reading the images out, Dr. Berger stimulates various parts of the brain to temporarily reduce their functionality, and he carefully observes how this stimulation affects the patient's ability to identify images and speak. The mapping process allows Dr. Berger to identify regions of the brain that don't correspond with any functionality that will visibly impair the patient if they are removed, so he begins moving toward the brain tumor by making a hole in this region of the brain. He continues testing the patient continuously as he makes the hole deeper, and he changes the hole's direction if necessary if he encounters brain tissue that he discovers is connected to motor or language function. All regions of the brain are responsible for something, so some damage is inevitable in this type of surgery, but by avoiding regions that correspond to motor or language function, Dr. Berger can minimize the damage from the surgery. He can also personalize this surgery further: he once had a math teacher do problems as he was having brain surgery so that Dr. Berger could avoid the most math-focused regions of his brain. This is a fascinating and innovative method of surgery! It's amazing that brain surgery can be effectively performed on a patient who is awake. This method allows the surgeon to dynamically adjust the pathway to the patient's brain tumor based on the patient's individual brain structure, which can be determined by talking with them during surgery. Interestingly, Dr. Berger discussed that there is considerable variation between patients when it comes to brain structure, so each surgery must be performed with great care. Dr. Berger reported that he has had excellent success rates with this surgery, and he continues to train neurosurgery residents at UC San Francisco to perform this innovative type of brain surgery. This was my last day at Barrow, so after doing a bit more research in the lab, I turned in my badge to Sarah, ubered to the airport, and flew home. This was an amazing experience, and I'm tremendously grateful to all who made it possible, including Dr. Michael Bohl, Jessica Bohl, and Sarah McBryan! My prototyping adventures brought me to an unusual place today: the cadaver fridge. (I was unable to photograph the location.) I needed a large space in which to cool my prototype, so Dr. Bohl led me up to the giant fridge to place my model inside. When we took the model out later, it was cooled to my satisfaction, which allowed me to continue testing it. While we were upstairs, Dr. Bohl let me see another interesting project he is working on. As part of the super-realistic experience he seeks to provide users of Spine STUD models, he wants to incorporate x-ray functionality into the models. However, the material that the bone of the models is made of appears lighter than the muscle material on an x-ray, which is not realistic. For reference, here is what an actual x-ray looks like:  It's easy to see that the cervical spine in the person's neck is visible much more sharply than the muscle. To provide a realistic experience, this is what Dr. Bohl seeks to replicate. In the lab, Dr. Bohl tried adding a certain material to the bone model, and he brought the model up to the x-ray machine to try out x-raying it. Unfortunately, he didn't have any synthetic muscle ready, but his addition of the material to the bone model significantly improved x-ray visibility, as can be seen in the picture below. 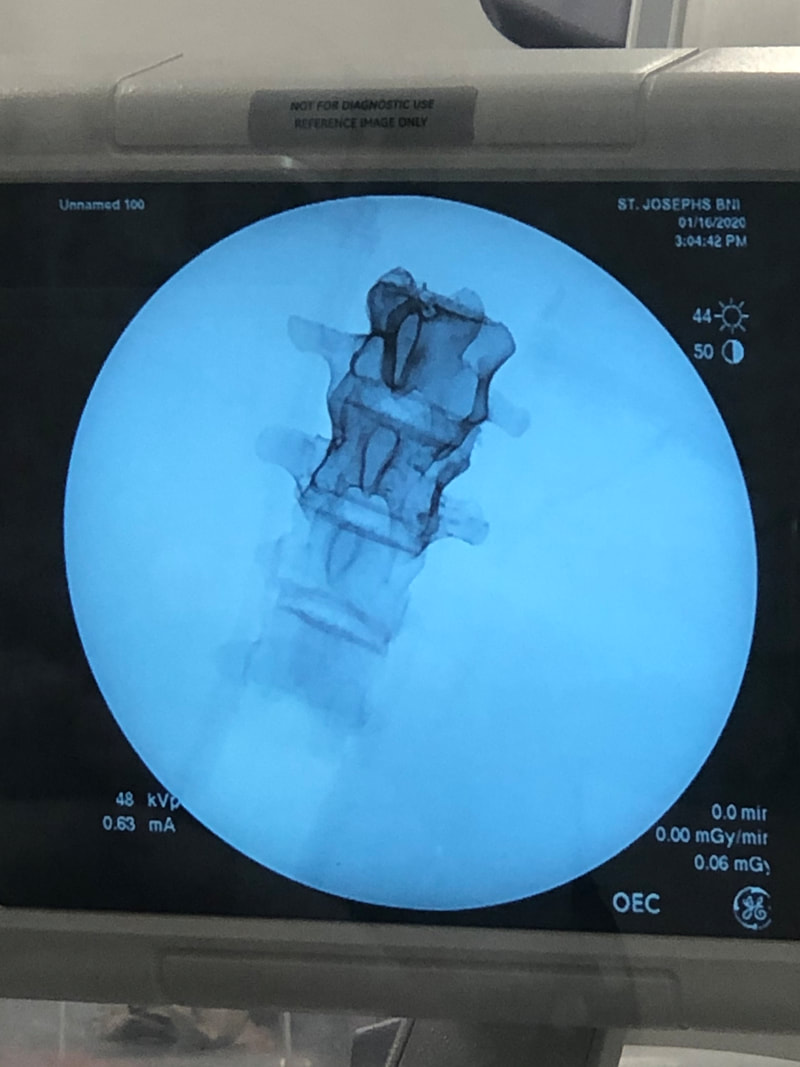 The part of the spine with the special material added is extremely clear! The top part has the material added, while the bottom part doesn't. It's easy to see why the bottom part is hard to see inside a complete, life-like model. When synthetic muscle surrounds the top part of the spine, it should be quite easy to see the bone through the muscle. This will allow training surgeons to x-ray a model to generate imagery and determine details about the model's condition, which will allow training surgeons to perform a more precise surgery tailored to the "needs" of the specific model. This is precisely what real surgeons do with patients, so this model should ultimately lead to more effectively trained surgeons. Another very cool thing that I got to see today at a demo in the hospital was a surgery robot called the DaVinci robot. This is a robot that assists surgeons in performing minimally invasive surgery by transforming a surgeon's actions into much more subtle and precise movements. The surgeon sits at a control panel and operates the machine using both hands and an eyepiece that provides a 3D view of the surgical situation. Below is an image of the complete robot.  It's a very complex robot, and it costs over $2 million! However, it offers fascinating functionality to surgeons. Below is a closer look at its arms. 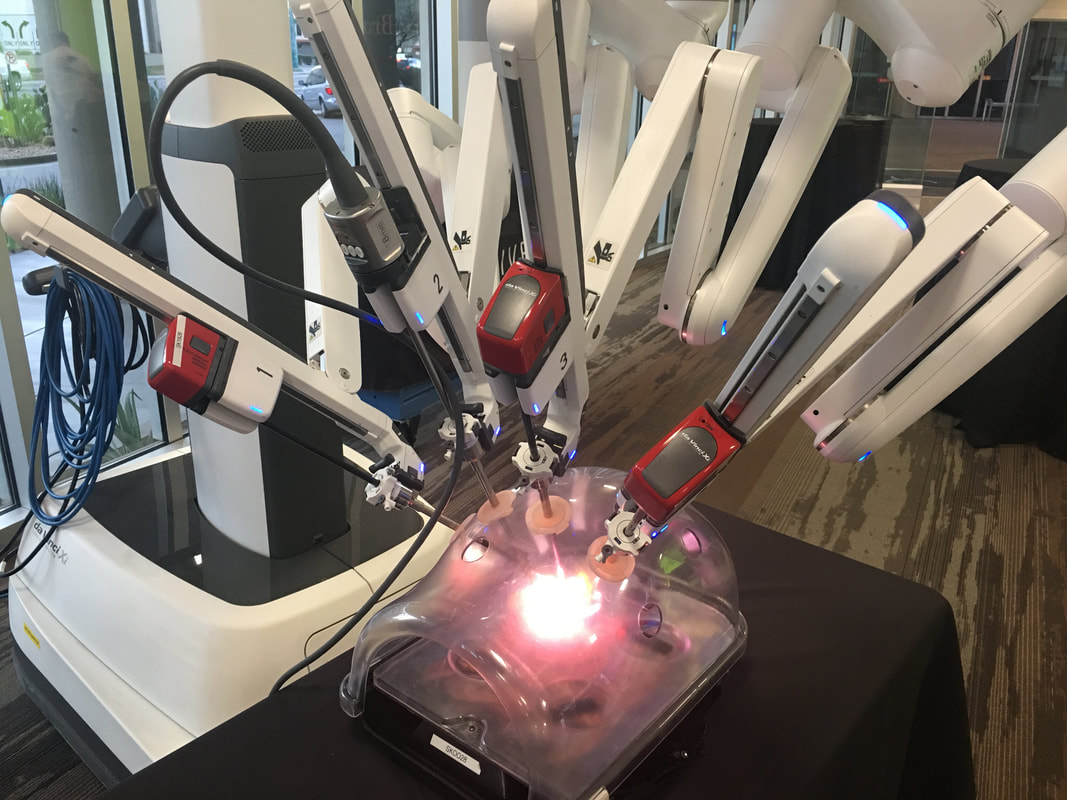 The surgeon can use foot pedals to switch between the arms during the surgery. Each arm is equipped with a grabbing mechanism and a light, which the surgeon can control from the control station below. Each arm is also equipped with electrocautery functionality, which is when an electrical current is sent through a conducting material to seal broken blood vessels. It's basically branding on a miniscule scale, and it's extremely helpful for surgery. The electrocautery is opperated with the top left pedal below.  I got to try out the device on a physically attached model that allowed me to test the device's maneuverability, and it felt very intuitive! I looked through both eyepieces, which provided a 3D view of what I was doing. I used the two hand pieces that can be seen above to operate the arms, and I simply moved my hands around very naturally as if I were moving my hands around the landscape that I saw. To close the grabbers, I just closed my fingers, and I found it very easy to move the small rings around the pegs. In addition, the machine provided haptic feedback, so it felt almost like I was actually touching the landscape I was operating on. Overall, it was a very cool experience!
I did some more research on this device, and it has received some criticism for being a solution in search of a problem and not actually improving patient outcomes. Still, the device offers some very interesting options to further expand the field of neurosurgery, and one area I would be especially interested in looking into is the integration of AI and machine learning with this kind of system. I'm sure computer vision algorithms could be developed to perform some tasks with this machine, and a variety of AI techniques could likely also be used. AI could first be implemented in some very specified tasks, or even just to help surgeons avoid mistakes, understand anatomy, remember steps, or otherwise boost their capabilities. Of course, it will be a long time before people are ready to let machines operate on them with minimal or no supervision by a human surgeon, but it would be a fascinating area to explore! As usual, I spent most of my day working on the ultrasound model. I tried experimenting with some odd new materials, and I've had some intriguing results! One fun thing about developing new technology is that sometimes the most surprising materials can be the most effective. It's very fun to be in a lab like this one where nearly anything scientific I want to do is possible: I can heat things, cool things, vacuum things, inject air, use a wide variety of chemicals, 3D print things, and more.
Another thing I began today was a project in which I work with data! Data science is one of my biggest interests, and I've been studying it independently for over a year now, so I was extremely excited to get a chance to provide helpful services with data. The first step in any data science project is to understand the data. This data is a confidential dataset of every operation that took place in the hospital between mid 2017 and 2019, and it was provided to me by Dr. John Sheehy. The first thing I'm investigating is overlapping surgery. After talking with Dr. Sheehy and Dr. Bohl about overlapping surgery, I read this article to gain a better understanding of the practice and criticisms of it, which I summarize below. Overlapping surgery is when one senior surgeon (known as the attending) supervises two cases at the same time. Much of the mechanical work on a surgery is performed by residents, and the attending is only in the room for the most technical parts. According to every surgeon I've talked to, this practice allows more surgeries to happen while also giving residents real-world training in surgery without the attending standing over them. This both allows more people to access care more cheaply and leads to better trained surgeons in the future, since with overlapping surgeries, and resident's first experience working alone occurs before they become an attending. However, this Boston Globe article alleges that overlapping surgeries decrease the quality of surgery. The article references several individual cases in great detail to stir up emotion but provides little effective data to support its allegation. Unfortunately, this article provoked tremendous public backlash against overlapping surgery, and federal laws were nearly passed that would ban the practice. Almost all doctors were outraged that the practice was nearly banned, because they are in almost unanimous agreement that the positives of overlapping surgery outweigh the risks. My job is to help answer this question - using an actual, massive dataset. My first task is to make a new column for each row (which represents a surgery) that contains the fraction of the surgery that overlaps with another surgery supervised by the same attending. For instance, if an attending is also working on another surgery for half the time they're working on one surgery, the overlap_fraction column's value for that row would be 0.5. Dr. Sheehy says that he currently has a way to figure this out in excel, but it takes a whopping 48 hours for his computer to calculate the solution. This is a situation in which more versatile data analysis tools like python and pandas are superior, because they aren't encumbered with loading the data graphically for all operations, and they offer the user far more functions. This is one thing I'll work on when I get back to school next week, and it will be a great way for me to test my data cleaning skills! One of the most interesting things I got to witness today was a business meeting about the future of Spine STUD. The details of the meeting are confidential, but I can discuss some general topics that were talked about and what I learned from them.
The people present at the meeting were Dr. Bohl, Sarah, me, a patent attorney, and Ray Thurston, who helps manage the company. The first part of the meeting was all about patent law. Since Spine STUD is generating many innovative new designs for surgical training devices, there are many design details that Spine STUD seeks to patent. However, patenting things is an extensive and bureaucratic process, so Spine STUD's small and busy team isn't always able to patent things the moment they are invented. The patent attorney repeatedly stressed the importance of promptly patenting things so that competitors don't rip off Spine STUD. Another thing the patent attorney stressed was the importance of extensive documentation. To file a patent, every tiny part of the invention must be documented and described, including exactly how it is made. Patent filers also must provide an extensive list of sources that they consulted for ideas when making the invention. This list of sources becomes essential in an intellectual property infringement lawsuit. The plaintiff party almost always subpoenas all of the R&D files relating to the invention, including browser search history and emails within the company. If any of these files reference a resource that is not included in the list of sources, then the plaintiff can make an argument that the defendant relied on someone else's work and didn't cite it. Even if the resource wasn't actually critical in the development of the invention, the plaintiff can still argue to the judge that it was, so these lawsuits can be extremely expensive and time-consuming. Especially for a small company that doesn't have the resources to defend itself from many lawsuits by big companies, it's critical that this list of sources be as airtight as possible. International patents were another topic that were discussed. Based on what I heard, it sounds extremely difficult to enforce a patent overseas! This is due to a wide variety of factors. One such factor is that overseas courts are often blatantly biased toward parties from the nation that the court is in, which makes getting a fair trial for infringement unlikely. This is especially true in developing countries like China, where the government is more concerned with promoting economic development than upholding barely-enforced international intellectual property standards. Another reason that securing international patents is difficult is because companies usually have to pay individually for every patent they hold overseas. In some cases, as the patent attorney explained, companies can end up paying millions of dollars to hold on to international patents that they hardly, if ever, use. The payoff for patents comes when they are infringed upon, Depending on the details of the infringement, patent holders can receive up to hundreds of millions of dollars. For a small company, this can be more than their revenue over the course of decades, so companies who file patents actually hope that their patent will be infringed upon so that they can collect damages. Many companies conclude that the best strategy is to focus only on the US for patents, since paying for US patents only is more reasonable than paying for many international patents, and US patents (along with patents from several other English-speaking nations and European nations) are most likely to be fairly enforced. I got to watch part of a surgery today! Unfortunately, I can't actually enter the operating room (OR), since I'm under 18. However, another 7th year resident named Dr. Sheehy kindly logged into the surgery camera network and showed me some surgeries that were taking place. All of the hospital's OR cameras are connected to a single network, so any doctor can log in and watch surgeries. We logged in at a good time, because a brain surgery was taking place. In fact, Dr. Bohl was helping perform the brain surgery we watched.
There were several different views of the surgery available. The first view we looked at was a magnified view of the incision, in which we could see several tools probing around the brain. Based on the way in which the tools were moving, Dr. Sheehy immediately identified the surgeon as left-handed, which meant that the surgeon was most likely Dr. Lawton, a senior neurosurgeon at Barrow. Dr. Lawton was slowly descending deeper and deeper into the brain, and Dr. Sheehy explained that the goal of this surgery was to treat a ruptured mycotic aneurism. An aneurism occurs when a small area of a blood vessel in the brain becomes weak, which causes that area to balloon as blood presses against it. These blood vessel balloons are known as aneurisms, which can rupture, causing potentially catastrophic damage to brain tissue. Unfortunately, this patient had an aneurism that ruptured, so the surgeons were doing everything they could to mitigate the damage. However, this ruptured aneurism wasn't just any ordinary aneurism; it was a mycotic aneurism, which means that it was infected with bacteria. Such aneurisms often occur in drug users who share needles, but they can also occur in otherwise healthy people. Unsurprisingly, mycotic aneurisms are even more difficult to treat than regular aneurisms if they rupture. This aneurism was quite deep in the brain, so Dr. Sheehy explained that the easiest way to access it was to go between the temporal lobe and the parietal lobe. There is a deep crease between these two lobes, so it's possible to squeeze between the lobes without making any incisions. It's amazing how much the brain can be pushed around if it's pushed gently enough! The other view I got to see was the view of the entire OR. There were several people in the OR, including Dr. Lawton, Dr. Bohl, the anesthesiologist, and several scrub nurses who were helping with the surgery by retrieving tools, monitoring the patient, and performing other similarly essential tasks. Dr. Sheehy explained that assistants like scrub nurses have to "scrub in" to the operating room, which means that they wash their hands up to their elbows (scrubbing thoroughly, of course) and put on sterile surgical attire. In fact, this is how the term for standard hospital attire, scrubs, originated. The anesthesiologist kept a close eye on the patient's condition to balance sedation with organ activity. Dr. Bohl performed parts of the surgery with Dr. Lawton's supervision, but since this was a challenging and serious case, Dr. Lawton performed much of the surgery as well. Interestingly, almost all the equipment in the OR was mounted on wheels, so if there wasn't a patient in the OR, the entire room could probably be cleared of equipment in less than a minute. This mobility allows the hospital to buy a wider variety of specialized equipment, since they can move a limited number of each type of specialized machine between rooms as necessary. Although it would have been great to step inside the operating room for real, I still enjoyed this glimpse into how an operating room operates. There are some great places to run in Phoenix!     I spent much of today testing the electrical functionality that I started experimenting with yesterday, and I constructed my first working prototype of it today! Again, since this functionality will likely be patented, I can't go into detail about it. Overall, I feel like I'm developing a much clearer sense of the process of scientific testing and iteration by working on this model. I got to do another surgery on the model today! This time, I got to do a laminectomy, which is a surgery in which the dorsal part of a vertebra, called the spinous process, is removed to relieve pressure on nerves. The circled part of the photo below is the spinous process, which is the part that is removed in a laminectomy. 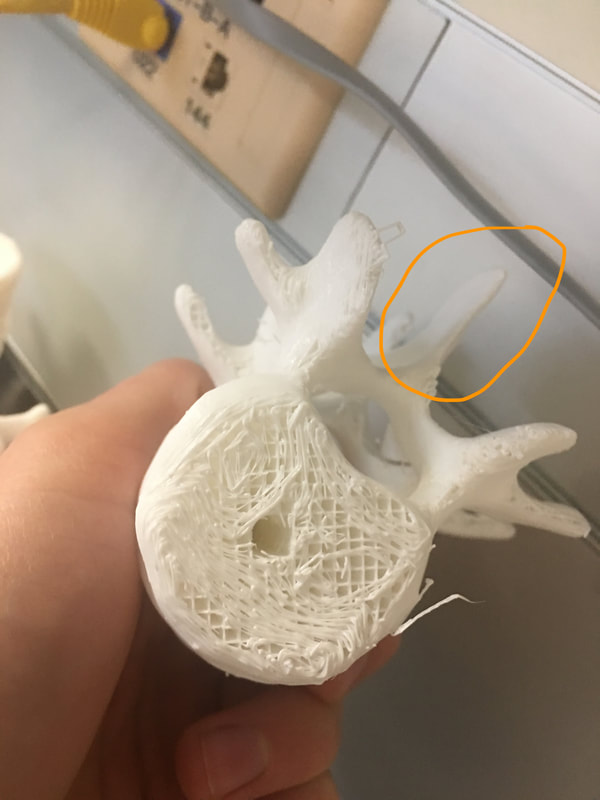 Below is a photo of a 3D printed model of the spine to put this vertebra in context. The part that my finger is on is the spinous process of a single vertebra, which is what is removed in a laminectomy. 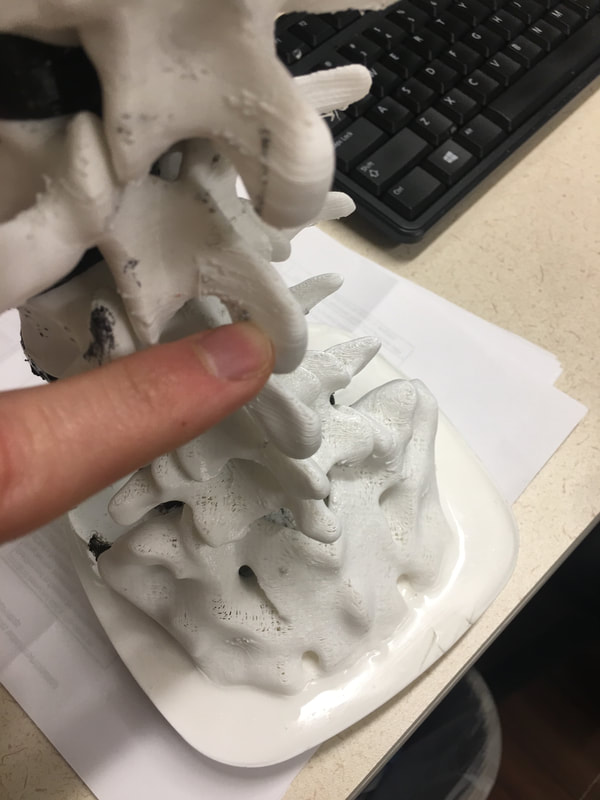 I did the procedure on the same model that I used yesterday for the screws. The end result is visible in the image below, and the space of the spinous process that I removed is visible inside the green circle.  If you look in the center and on the right, you can see that this isn't the first laminectomy the model has had! The first step of a laminectomy is to rip out the spinous process using the tool below. I also had to rip off the transverse processes, which are the "wings" coming off either side of the spine. I had to squeeze the tool quite forcefully when ripping the bone out, but Dr. Bohl assured me that this wouldn't hurt the patient. It's amazing that the human body can tolerate having whole bones removed if the procedure is done correctly! 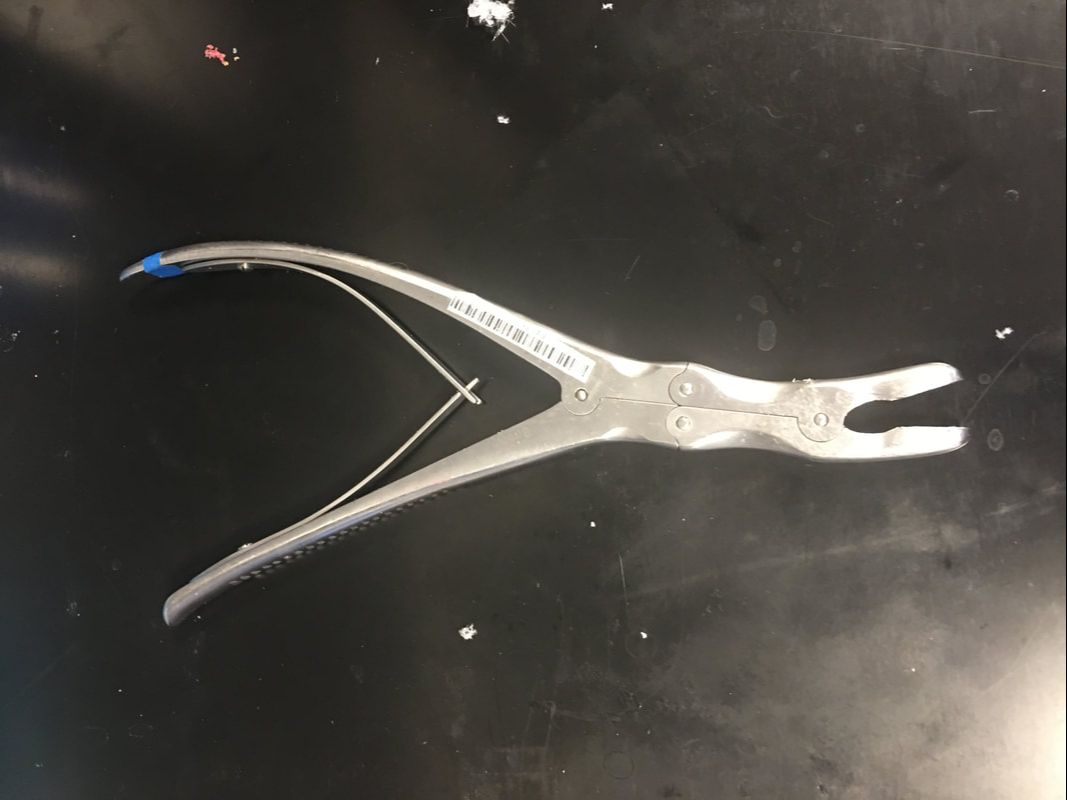 The key when using the tool above is to squeeze, not to pull. If I squeezed hard on the handles, the wrench would crush the bone, making it easy to remove. On the other hand, if I simply grabbed the bone and pulled, the entire spine would move, which could damage other parts of the spine. Once the large parts of the vertebra were removed, the fecal sac, which is a thin membrane that runs down the entire length of the spine, became exposed. One major challenge of performing a laminectomy is avoiding the fecal sac. It's very easy to puncture it when ripping out the soft bone that closely surrounds it, so like the last surgery, I had to use great caution when working near it. There exists a special tool designed to take out small chunks of bone near the fecal sac, which is shown below.  This tool can get under parts of the vertebra to bone that would be inaccessible to the large wrench shown above. Like the wrench above, the key when using the tool is to squeeze the handles forcefully. I ended up with a small pile of bone fragments, so I asked what surgeons did with bone fragments in the real OR. Interestingly, Dr. Bohl said that they grind up the fragments and sprinkle them around the areas of bone that they operated on, which helps the bone naturally repair itself. This makes sense based on what I remember learning in AP Biology last year. Bones have cells called osteoblasts inside them, which secrete minerals (especially calcium) and collagen to form the bone. There are still living osteoblasts in bone dust, so sprinkling the dust into damaged bone would be like providing troop reinforcements for reconstructing bone. Fortunately, I managed to complete the laminectomy without damaging the fecal sac! However, I wanted to experience repairing the fecal sac, so Dr. Bohl made a small hole in the fecal sac of the model to simulate puncturing it during surgery. If the fecal sac is punctured, a stream of liquid will squirt up into the surgeon's face, and they will have to quickly sew the sac back together. Dr. Bohl made sure that we both stood back when he punctured the fecal sac, because a stream of water did indeed squirt out! A special thread exists to sew the fecal sac back together, which is shown below. 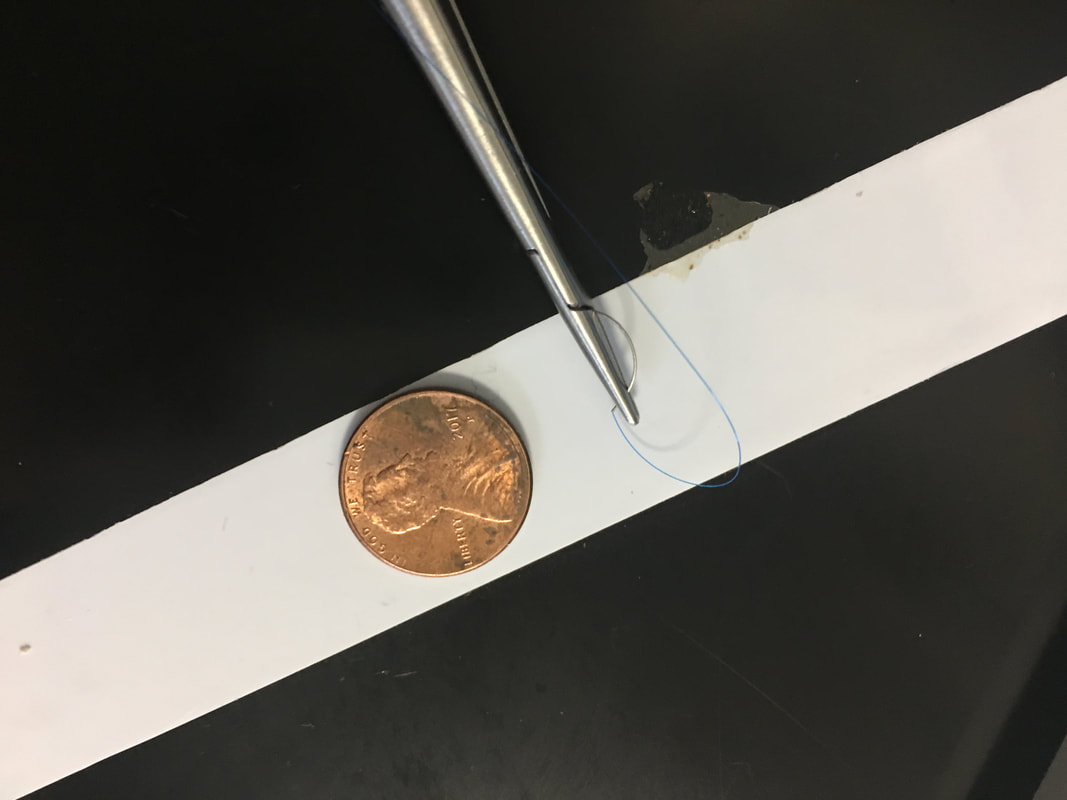 A tiny needle is visible on one end of the thread, which is used to drive the thread through the wall of the fecal sac. There is a special tool used to manipulate the thread, which is also shown above. To sew together the ruptured fecal sac, I had to use a variety of knots that Dr. Bohl taught me earlier today. Interestingly, I could use my hands to make many of the knots, because I made them near the top of the string and pulled them down to the fecal sac. However, there are also some knots that must be made with only the instrument above, because these knots require considerable precision. Tying knots is an important skill to have in many areas of surgery, because knots are required almost anywhere an incision is required. When I finished tying the knots, I used the tool below to reach down into the model and cut the string close to the knot. 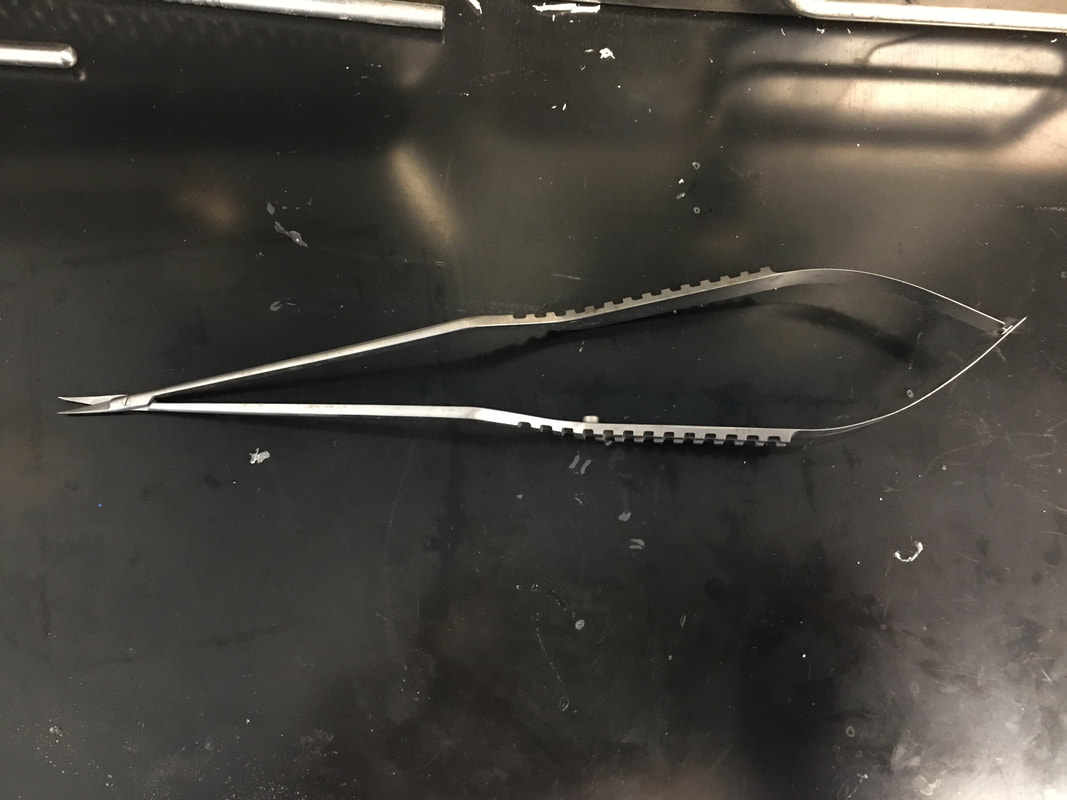 After my first round of stitching, I squeezed the fecal sac to make sure that the puncture was sealed. Unfortunately, water continued to leak out, so the knot wasn't in quite the right place to be effective alone. I made several more knots in the same way around the puncture point to finish sealing the fecal sac.
It's crucial that the fecal sac isn't leaking when the patient is stitched back together, because the fluid in the fecal sac prevents the bone from healing if it leaks. This delay in healing can lead to further complications (especially bacterial infections), and in the worst cases, it can lead to the death of the patient. It's equally important to ensure that there are no bone fragments remaining from the laminectomy that can puncture the fecal sac when the patient moves after the surgery. If the fecal sac is punctured after the surgery is over, the patient usually has to undergo surgery again. Though the laminectomy is considered a relatively basic spine surgery, it's essential to perform it carefully to avoid complications. |
Jeremy MahoneyI'm a high school student at Maumee Valley Country Day School, and I'm currently doing a neurosurgery-focused independent study at Barrow with Dr. Michael Bohl. ArchivesCategories |
 RSS Feed
RSS Feed
